


Study
Health inequality increased sixfold in South Africa under Covid-19, suggesting that the crisis affected the health of the poor far more than the relatively well-off. Race is not a significant predictor of vaccine hesitancy, but trusting social media as an information source is positively correlated with vaccine hesitancy. South Africa has pushed hard against opposition to the proposal for a waiver of IP for Covid-19 technologies at the World Trade Organisation (WTO).

This study is part of the series "No one is safe until everyone is safe - Global perspectives on Covid-19 vaccination" by the Heinrich-Böll-Stiftung's European Union and Washington, DC offices.

Download the study "Global perspectives on Covid-19 vaccination - COVID-19 Vaccine Distribution in South Africa" by Lauren Paremoer and Leslie London
Background
On 2 March 2020, the National Institute of Communicable Disease (NICD) in South Africa confirmed the first recorded case of COVID-19 in South Africa. Between 26 March and 16 April 2020, the country suspended all but essential services and severely restricted movement. Subsequently, the country has experienced two waves, i.e. periods of intense transmission starting from a weekly incidence of 30 cases per 100,000 up until peak weekly incidence. The first wave occurred between weeks 24 and 28 of 2020, and the second from week 47 of 2020 until week 1 of 2021. By 8 May 2021, South Africa had experienced a total of 1,595,817 confirmed cases of COVID-19 and 54,724 deaths, with a recovery rate of 94.9%.
A significant proportion of mortality due to the epidemic is not reflected in official statistics because people may die from COVID-19 before they get to a facility or being diagnosed. The South African Medical Research Council (SAMRC) estimates that by 1 May 2021, 157,542 more deaths were occurring as a result of the epidemic. Of these, between 85% and 95% (or between 133,911 and 149,665) deaths are estimated to be due to COVID-19, meaning official statistics reported only about 36% of COVID-19 deaths in the country.
COVID-19 amongst health workers
A press report from 16 November 2020, cites the Minister of Health as indicating a total of 35,490 “healthcare workers” had “been infected” with COVID-19 at that point, but does not explicitly indicate that this figure contains both public and private sector workers. According to the National Institute for Occupational Health (NIOH), 330 healthcare workers died during the first wave, and 423 during the second wave. The fact that there is no accurate database of health worker infections with COVID-19 is a reflection of weak occupational health systems in the health sector prior to COVID-19, which are only partially being addressed in the current epidemic response.
Very little data has been published regarding COVID-19 prevalence rates amongst community health workers (CHWs) and allied health workers (e.g. porters). In mid-March 2021, the NIOH reported that of the 6,758 workers admitted to hospital for COVID-19 to that date, 59.8% were nurses, 21.7% porters or administrators, 8.6% allied health workers, 6.7% doctors, 2.4% paramedics and 1% laboratory scientists.
Health system capacity constraints
Throughout 2020, provincial health departments engaged in efforts to bolster access to critical care beds through concluding service level agreements (SLAs) with private sector hospitals. These complex negotiations proceeded on a province-by-province basis and in the end only one province – the Western Cape – successfully concluded an SLA with the private sector (there was little need for using it as the public sector was able to manage its patient load).
Community health workers are the foundation of the South African health care system and deliver primary health care to households in South Africa’s most marginalised communities, comprising of preventative, promotive, curative, rehabilitative and palliative services. CHWs are typically poorly and irregularly paid, and have no employee benefits. The government has relied on the labour of CHWs in COVID-19 prevention, education and monitoring efforts, but has not always provided them with adequate personal protective equipment (PPE) or training. Despite the expectation of a third wave, the National Department of Health (NDoH) is still ambivalent about in-sourcing CHWs, as their exploitative terms of service have not been addressed during the pandemic. In some provinces, for example the Eastern Cape, CHWs have been fighting retrenchments after the provincial government claimed it had run out of funds to pay them in March 2021. Locally-trained doctors also experience problems in finding posts and with salary payments as a result of dysfunctional health services in some provinces.
Economic effects of the COVID-19 pandemic
The recent Corona Virus Rapid Mobile survey showed that health inequality increased sixfold in South Africa under COVID-19, suggesting that the crisis affected the health of the poor far more than the relatively well-off. During the first and second quarters of 2020, which coincided with South Africa’s hard lockdown, GDP fell by just over 16% and household spending dropped by 49.8%. Women made up two-thirds of those who lost their jobs between February and April 2020. According to a recent United National Development Programme (UNDP) report, many households that had been positioned on or just above the poverty line prior to the pandemic are likely to fall into poverty. It projects that “about 54 percent of households pushed out of permanent employment to informal jobs are likely to fall into poverty, about 34 percent of those categorized as middle class are also likely to fall into vulnerability or poverty.” Households that depended on employed relatives or friends to subsidise their income saw this disappear in the context of the three million job losses suffered during the first half of 2020.
Since March 2020, the national government implemented almost 1,200 social protection measures aimed at alleviating the effects of COVID-19, which provided support to 63% of the population. Cash transfer schemes constituted a third of these measures. The government introduced a special COVID-19 social relief of distress (SRD) grant worth R350 in March 2020. By September 2020, it had reached 4.3 million recipients (12% of the adult population); 33% of recipients live in the poorest quintile of households. Civil society organisations (CSOs) have called for it to remain in place until the government introduces a basic income scheme, that its value be increased to the food poverty line of R585, and that recipients of the child grant (95% of whom are women) are deemed eligible to receive the grant. The COVID-19 SRD is not available to people already receiving social grants. Thus, women already receiving relatively modest childcare grants have been refused access to this grant (55% of the SRD grant recipients are men).
Much of the government’s COVID-19 relief spending has been financed through loans. In July 2020, South Africa took out a loan of $4.3 billion (or R70 billion, based on exchange rates at the time), at an interest rate of 1.1%. Critics have argued that the loan may be based on an implicit understanding that the government should implement austerity policies, and that it might be difficult to repay if the rand devalues. The government has also taken out loans with the New Development Bank ($1 billion or R16.5 billion at the time) and the African Development Bank ($288 million or R5 billion at the time).
Vaccine Rollout
Timelines for the vaccine rollout
On 3 January 2021, the government announced its vaccination rollout strategy. Phase 1 of the rollout strategy aims to vaccinate 1.5 million healthcare workers from February to April 2021. Vaccinations commenced on 18 February, but, in the absence of a registered vaccine in South Africa, the programme was included in the implementation arm of a Johnson & Johnson (J&J) vaccine trial. By 22 April 2021, an estimated total of 292,623 health care workers had been vaccinated.
Registration for Phase 2 of the vaccination process, targeting persons 60 years and older, opened during the second week of April. The government has made available an online registration portal and established a COVID-19 hotline, and has also promised to establish mobile outreach teams, a WhatsApp service and in-person registration at vaccination centres to assist people with limited internet access to register. Phase 3 aims to vaccinate the remainder of the adult population (about 22 million people) during November 2021 to February 2022.
Vaccine procurement: major suppliers
Vaccine procurement is being managed by the NDoH. The private sector – including private medical schemes – have indicated that they are willing to assist with financing procurement and implementing the rollout of vaccines under national guidelines. The bulk of South Africa’s vaccines are being supplied by Pfizer (30 million doses to cover 15 million people) and Johnson & Johnson (31 million doses). The J&J vaccines were obtained at $10 per vaccine, with no refunds should the order be cancelled, and subject to J&J receiving a letter from the Department of Trade and Industry (DTI) endorsing the local investment the company had made in Aspen Pharmaceuticals. Furthermore, the government was required to create a compensation fund by which it would indemnify J&J and assume state liability for any vaccine-related injuries. It is estimated that the fund could cost as much as R250 million in the first year. The Pfizer vaccines were also sold to the NDoH at $10 per dose, and this deal too is subject to indemnity and no-fault compensation requirements. Pfizer initially demanded that the South African government use sovereign assets as guarantees against the costs of any future legal cases stemming from vaccine-related injuries but later dropped this demand. It has reportedly tried to impose this demand on several countries seeking to secure a supply of its vaccines.
On 5 January 2021, Pfizer submitted its dossier with South African Health Products Regulatory Authority (SAHPRA) for regulatory approval; Section 21 regulatory approval, which allows SAHPRA to provide access to health technologies on an exceptional basis, was obtained on 16 March 2021. On 12 February, SAHPRA provided urgent study approval for the J&J vaccine; under the Sisonke Implementation Study, the J&J vaccine was rolled out from 17 January as part of a broader effort to enable the vaccination of South African health workers. On 14 April 2021, rollout of the J&J vaccine was briefly paused due to concerns about very rare side effects involving low platelet levels and blood clots. This decision was based on reports of these side effects in the USA, though none of these side-effects had been reported by South African trial participants. On 19 April, SAHPRA recommended that the trial be recommenced, but that screening and monitoring of participants at high risk for blood clots be implemented, consent forms updated to include this rare side effect, and clinical treatment be available immediately should such side-effect occur.
Vaccine procurement: smaller suppliers
The NDoH has secured smaller quantities of vaccines through a bilateral agreement with the Serum Institute of India (1.5 million doses of the AstraZeneca vaccine, given Section 21 approval by SAHPRA on 22 January 2021), COVAX (to cover 10% of South Africa’s population), and the African Vaccine Acquisitions Task Team (AVATT). The COVAX vaccines are secured through a “Committed Purchase” arrangement, which does not allow countries to opt out of using a specific vaccine, and was secured after the Solidarity Fund, a private sector funding platform, assisted the government with paying the deposit for South Africa’s allotment of vaccines. The COVAX process was intended to cover 10% of the population. However, subsequent bilateral agreements have vastly outnumbered the COVAX purchases, and it is thus unclear what role COVAX secured vaccines will play in South Africa's rollout. Given ongoing mutations in the virus causing COVID-19, it also remains unclear whether the vaccines secured through COVAX will prove efficacious against the dominant viral strains found in SA.
Other vaccine producers are also being engaged, including the manufacturers of the Sputnik V vaccine, Sinovac, Sinopharm and Moderna. However, at the time of writing, none of these engagements have yet delivered any agreement to purchases of these vaccines.
Procurement and concerns about lack of transparency
Payments for both COVAX and bilateral purchases were released through special approval from the National Treasury in 2020 and January 2021 to deviate from standard procurement procedures. This enabled the NDoH to waive standard, open-bidding procurement procedures so that it could contract directly with Pfizer, AstraZeneca, Moderna and Johnson & Johnson, or any other manufacturer that has vaccine stock available. The approval was granted on 6 January 2021, for a six-month period.
However, South Africa’s record on procurement generally during the COVID-19 epidemic is of some concern. During the early stages of the pandemic, procurement of PPE was decentralised to provincial governments, but this decentralisation was said to have played an important role in enabling corruption in PPE procurement. Perhaps due to concerns about corruption that marred the early PPE procurement, all procurement of PPE and other materials required to roll out the vaccine campaign will be the responsibility of the NDoH.
The Biovac Institute (Biovac) has been an important source of storage and distribution infrastructure in Phase 1 of the vaccine rollout. Biovac was established in 2003 as a public private partnership (PPP) between the NDoH and the Biovac Consortium to promote national vaccine manufacturing capacity. Between 2003 and 2018, Biovac had an exclusive agreement with the NDoH to procure, store and distribute vaccines for the national Expanded Programme on Immunisation (EPI). In 2018, this arrangement ended and the PPP was terminated. Biovac then became a joint venture between the Department of Science and Innovation (DSI) (which holds 35% of shares), the Technology Innovation Agency (an entity of the DSI which holds 12.5% of Biovac’s shares), and Immunotek. However, it remains the main supplier of vaccines to the NDoH, having secured 85% of a R11.4 billion tender to supply childhood vaccines from June 2020 to December 2023.
Single source contracting is being used to secure Biovac’s services for vaccine storage and distribution for the first three months of the rollout. Closed bids were issued to Biovac Institute, Imperial Health Sciences, DSV Global Transport and Logistics and United Pharmaceutical Distributors to provide these services for six months. It is unclear whether these six months start after the three months allocated to Biovac. Standard open bidding procedures were used to secure provision of importation and logistics services to support its vaccination programme from 1 April to 31 December 2021.
Local manufacturing and research capacity
Only two South African entities, Biovac and Aspen Pharmacare, a South African-owned global pharmaceutical company, are active in the vaccine production field. However, even if South Africa had more vaccine manufacturing capacity, TRIPS provisions inhibiting technology transfer and the slow pace of local patent law reform would still pose significant barriers to producing COVID-19 therapeutics locally. No South African institution currently has the capacity to produce active ingredients for vaccines at a commercial scale, though Biovac and some universities have know-how and physical infrastructure in this respect. Biovac could arguably develop this capacity if sufficient financial and human resources were invested in this, but it could cost as much as R8.9 billion (about $647 million using exchange rates from early June 2021) to do so.
Emerging capabilities for producing biologics, proteins for diagnostics and vaccines
The Council for Scientific and Industrial Research (CSIR) is developing a manufacturing facility at its Pretoria campus that will have the capacity to produce sufficient quantities of biologics for clinical trials, thereby hoping to eliminate the need to contract for this service with foreign companies. The University of Cape Town’s (UCT) Biopharming Unit has developed processes that use plant cell lines to manufacture protein-based therapeutics and vaccines, but has licensed this technology to overseas companies due to the absence of local manufacturing facilities. Two other entities, CSIR and AzarGen, are developing similar technologies for treating HIV, rabies and cancer. South Africa has had some success in producing proteins for locally and internationally manufactured COVID-19 diagnostics: CapeBio and Cape Bio Pharms, established with the support of CSIR and UCT respectively, are producing proteins for diagnostics and have developed a PCR test kit using local enzymes. This is seen as a significant first step towards producing proteins for use in therapeutics and vaccines. In December 2020, Cape Bio Pharms announced that the European Investment Bank (EIB) had granted it a R900 million loan to establish a facility in Mauritius. It will be named Cape Biologix and function as a subsidiary of Cape Bio Pharms, which would produce plant-based therapeutics and vaccines. Spotlight, an online publication published by Treatment Action Campaign and SECTION27 that specialises in health reporting, reports that “Cape Bio Pharms initially sought to secure funding to construct a facility in South Africa, but that South Africa was not eligible to receive the loan secured by Cape Bio Pharms from EIB” and that the Department of Science and Innovation “did not respond to requests for comment on the challenges faced by South African companies in securing financing for localisation of manufacturing capacity and the role that government can play in addressing this financing gap.”
“Filling and finishing” COVID-19 vaccines
Some South African pharmaceutical plants have fill and finish capacity, namely the capacity to fill vaccine vials and finish the packing of the vaccines. In June 2020, Biovac CEO, Dr Morena Makhoane, told Parliamentarians that Biovac could develop the capacity to fill and finish 10 million vials and 12 million pre-filled syringes of COVID-19 vaccines within 12 to 18 months if it could secure a technology transfer arrangement with an international manufacturer. In October and November 2020, it was reported that Biovac was involved in discussions with the Coalition for Epidemic Preparedness Innovation (CEPI) and an undisclosed international manufacturer to manufacture components of COVID-19 vaccines, but by January 2021, no agreements to this effect had been publicly announced. In March 2021, Spotlight reported that Biovac had recently concluded a technology transfer arrangement with ImmunityBio, an American company, to manufacture its COVID-19 viral vector.
Capability to produce non-COVID vaccines locally
In November 2020, Biovac announced that it would soon begin local production of a combination vaccine (Hexaxim) effective for diphtheria, tetanus, pertussis, Haemophilus influenzae type b, hepatitis B and polio, with the aim of filling 4 million doses in 2021. In January 2021, Biovac announced it would start producing a vaccine for preventing pneumococcal infection in children, Prevenar-13, within six months, using components provided by Pfizer. Aspen Pharmacare has secured a contract with J&J to fill and finish their COVID-19 vaccine. It has a much larger fill and finish capacity than Biovac (Aspen can produce 300 million doses per year). Nine million doses of the vaccine will be allocated for domestic use, though this guarantee was only secured in January 2021, after pressure on J&J to allocate a portion to the SA market.
Vaccine trials
South Africa has a strong biomedical research infrastructure, and three vaccines have been trialled locally: the AstraZeneca Phase IIb trial (started in June 2020); the Johnson & Johnson first Phase III COVID-19 vaccine trial; and the Novavax Phase IIb trial (the latter two both started in September 2020). These trials have the advantage of helping to determine the efficacy of vaccines to local variants of COVID-19. Trials of other agents are also in development. For example, in February 2021, a local immunotherapy company, Genlab, announced that a collaboration between it and a Danish biotechnology company (Immunitytrack) had led to the development of “the first Covid-19 vaccine of African origin, called Shantivax”. The company has indicated that the vaccine is undergoing pre-clinical testing, and that clinical trials for the vaccine will take place towards the end of 2021 or the start of 2022. SAHPRA has indicated that it has not received “any communication or applications for the vaccine.”
Lauren Paremoer on Covid-19 Vaccine Distribution in South Africa - Heinrich-Böll-Stiftung European Union
 Watch on YouTube
Watch on YouTube
Expected consequences of the vaccine deployment for the economic outlook in South Africa
Many publications have spoken to the economic effects of the pandemic, but less has been written on the projected economic benefits of the rollout. The South African Treasury has taken the position that the vaccine rollout is essential for securing the stability of the South African economy, but argues that by itself this intervention is likely to have significant benefits in terms of economic growth, job creation and greater equity in distribution of income and wealth. The 2020 Medium Term Budget Statement, released in October 2020, when South Africa had not yet actively pursued vaccine procurement, argued that any future vaccination campaign “would likely improve sentiment, productivity and growth in the short to medium term,” without quantifying the likely impact of the intervention. The February 2021 Budget Review positioned a mass vaccination campaign as “Government’s immediate priority” in order to “support a reopening of the economy and GDP growth of 3.3 per cent this year […] moderating to an average of 1.9 per cent in 2022 and 2023”. However, this document repeatedly argues that the economic outlook remains uncertain, even if the vaccination campaign should prove effective, and that unemployment, income loss and economic growth can best be secured through addressing South Africa’s “structural constraints”, which, according to the Treasury, consists of high “costs of doing business”, unreliable electricity supply, low investor confidence, weak labour markets, financially distressed public corporations, low consumer confidence and low capital spending by corporations. Worryingly, despite the deepening inequality, unemployment and poverty brought about by COVID-19, the Treasury has indicated that “[o]ver the next three years, annual debt-service payments [will] exceed government spending on most functions, including health, economic services, and peace and security.” Thus, even if the vaccination campaign should be effective – i.e. 67% coverage by the end of 2021 or start of 2022 – the proportion of national spending on social services will at best remain at current levels, despite deepening levels of socioeconomic vulnerability and increasing levels of inequality.
Vaccine Acceptance and Scepticism
Vaccines As a Human Right
Whereas the Intellectual Property Regime under the World Trade Organisation (WTO) treats vaccines as a commodity, the UN Committee on Economic, Social and Cultural Rights has clearly argued that access to a safe and effective vaccine for COVID-19 is an essential component of both the human right to health and the right to enjoy the benefits of scientific progress. As such, states have obligations, to the maximum of their available resources, to guarantee access to vaccines, without any discrimination. Moreover, the international dimensions of human rights imply that states have a duty of international cooperation to ensure access to COVID-19 vaccines. The Committee called clearly for States to support the proposals of the waiver, including by using their voting rights within the WTO.
Are vaccines mandatory?
COVID-19 vaccination will not be mandatory in South Africa and will be available free of charge to all adults, including non-citizens. Childhood vaccines are, strictly speaking, not mandatory, but children must have proof of vaccination to register for primary school. This policy has been able to maintain sufficiently high levels of population immunity for childhood infectious diseases.
Vaccination status regarding other diseases
Prior to the COVID-19 outbreak, South Africa had not attained the 95% vaccination coverage target for DPT immunisation recommended by the WHO, nor the 91% target set by the national government. The 2020 SAHR reports the following coverage rates for both sexes in 2019/2020:
|
BCG (tuberculosis) |
85% |
|
DTaP-IPV-Hip-HBV third dose (diphtheria, tetanus, pertussis (whooping cough), polio, Haemophilus influenzae type b (Hib), and hepatitis B) |
84.5% |
|
Measles second dose |
79.6% |
|
PCV third dose (pneumococcal disease) |
86.5% |
|
RV second dose (rotavirus) |
83.1% |
|
Immunisation coverage under one year |
83.5% |
According to press reports, the COVID-19 lockdown has negatively impacted childhood vaccination rates. In June 2020, Spotlight reported that national immunisation coverage dropped from 82% in April 2019 to 61% in April 2020; the coverage rate of the second dose of measles vaccine dropped from 77% to 55% in the same period. The North West (43%) and Western Cape (46%) provinces experienced the lowest rate of second dose measle coverage, and the Northern Cape (67%) and Mpumalanga (66%) were least affected.
Vaccine scepticism: fearing the vaccine vs fearing the virus
On 12 May 2021, Daily Maverick, an online newspaper, reported that South Africans are showing high rates of vaccine acceptance as “more than 71% of adults surveyed in the NIDS-CRAM Wave 4 study of Covid-19 impacts said they would get vaccinated if a jab was available” (visual representation of survey results included below).
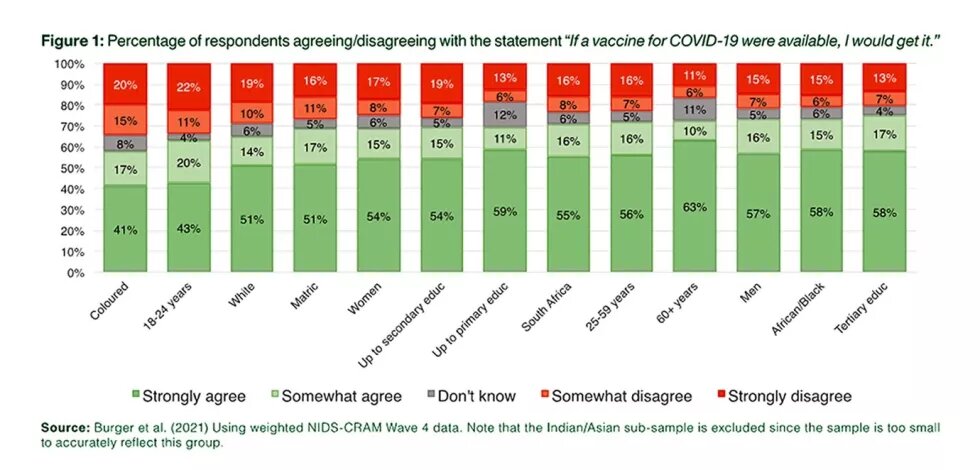
Source: Daily Maverick
According to the survey, elderly people and those with comorbidities were less likely to be vaccine hesitant than the youth and people with only a primary school education. Furthermore, race is not a significant predictor of vaccine hesitancy. Trusting social media as an information source is positively correlated with vaccine hesitancy. Reasons for vaccine hesitancy included fears about side-effects, doubts about vaccine efficacy, or “anti-vaxxer” beliefs.
Data from earlier surveys
An IPSOS survey conducted on 28 to 31 January 2021, in partnership with the World Economic Forum, surveyed a sample that it describes as “more urban, more educated, and/or more affluent than the general population. The survey results for these countries should be viewed as reflecting the views of the more ‘connected’ segment of their populations.” Despite this limitation, the data is presented as if it is broadly representative of the population in general, perhaps because the responses were weighted to reflect the demographic profile of the adult population, according to the most recent census data.
The IPSOS survey was conducted as South Africa reached the end of its second wave. It shows that in January 2021, 61% of “South Africans” indicated they were willing to take a vaccine if it should become available, up from 53% in December 2020. At the same time, 25% of South Africans “strongly disagreed” with the proposition that they would get a vaccine for COVID-19 if it were available to them, indicating significant resistance amongst some to being vaccinated. Amongst vaccine hesitant South Africans, 39% expressed concern about possible side effects, 33% were worried that clinical trials had moved too fast, 6% doubted the vaccines’ efficacy, 6% think their risk of contracting COVID-19 is too low to justify vaccination, and 9% “quoted anti-vaccination opinions as a reason” (“Other” reasons comprised the remaining 7%). The survey further reported that 47% of South Africans would support mandatory vaccinations for all adults, 50% opposed it and the remainder indicating that they “don’t know”.
An online HSRC survey was conducted during the height of the second wave (29 December 2020 to 6 January 2021) with 10,618 respondents. Findings are “broadly representative of the population at large” and responses were weighted by race, education and age. Overall, 67% of all adults are willing to take a vaccine if it becomes available, 18% said they would “definitely or probably not take a vaccine”, and 15% “did not know”. The two most frequently cited reasons for vaccine acceptance were protecting oneself (29%) and protecting others (25%), and the most common reasons for vaccine non-acceptance were concerns about side-effects (25%) and effectiveness (18%), “lack of trust in the vaccine, with little other explanation” (14%) and a lack of information about vaccines (10%). The survey shows that age, education and evaluation of government performance are correlated with “vaccine acceptance”, namely the willingness to be vaccinated:
- 71% of people that had “less than matric-level education” were willing to be vaccinated, compared to only 59% of people with a tertiary qualification.
- 74% of people aged 55% and older would take a vaccine compared to 63% of 18 to 24 year olds.
- Vaccine acceptance was 73% amongst respondents who thought President Ramaphosa was doing a good job, but only 36% among those who thought he was doing a bad or very bad job.
Amongst ordinary citizens from all walks of life, views are widely divergent, making it urgent to ensure access to information to empower people to make informed decisions about vaccines.
Disinformation about vaccines
In March 2020, the government gazetted regulations in line with the Disaster Management Act that made it a criminal offense to spread disinformation about the coronavirus pandemic. Despite this, social media has functioned as an outlet of disinformation about both the virus and COVID-19 vaccines. The HSRC survey discussed above identifies various misconceptions that help explain vaccine hesitancy in South Africa. This includes beliefs that the coronavirus doesn’t exist, that COVID-19 is not present in South Africa, that the vaccine is part of a conspiracy to control or harm people, or to address overpopulation. Some respondents believe the pandemic is caused by 5G towers, and that the vaccine will thus be ineffective. Others expressed concerns that the vaccine bears the mark of the devil and that it should thus be avoided by Christians.
Expectations Towards International Actors
Expectations towards the EU and USA
South Africa has pushed hard against opposition to the proposal for a waiver of IP for COVID-19 technologies at the World Trade Organisation (WTO), jointly proposed with India in October 2020, and now co-sponsored by more than 50 countries. South African officials in Geneva have lobbied the EU and US representatives at the WTO to support the waiver request. Locally, South African activists have generated support for the waiver proposal through peaceful protests in February 2021, outside embassies of countries opposing the waiver requests, newspaper opinion pieces, and a joint letter sent to senior US officials in January 2021, urging the Biden administration to use its political influence and proprietary rights to the Moderna vaccine to promote equitable access to COVID-19 vaccines globally. Activists have also placed pressure on the Norwegian government, which co-chairs the COVID-19 Act Accelerator alongside South Africa, to support the waiver request. International solidarity action by civil society networks appeared to have played an important role in shifting the Biden administration's position on the waiver, and in securing greater flexibility from key actors, such as the Norwegian Minister of Development, through engagement by civil society partners from Norway and South Africa. It is not clear what engagements Pretoria-based officials have had with the EU and US around vaccine access.
At a recent Africa CDC summit on building local vaccine manufacturing capacity, government officials across the continent, including those from South Africa, signalled that they would welcome foreign investment aimed at building local pharmaceutical production capacity. However, no explicit guarantees of state subsidies, tax exemptions, favourable loans or other incentives for private investors were promised at the conference, nor was there any explicit commitment to subordinating national political interest for a common African position. Most of the for-profit corporations who were given a platform to speak at the conference were from the global north (e.g. J&J, Moderna, GSK and Samsung Biologics), though some African (Aspen Pharmacare) and Indian (Bharat Biotech) firms gave inputs.
Expectations towards China and Russia
Geopolitics will likely play an important role in who provides vaccines and vaccine-related technology for populations in the continent and in South Africa. Both Chinese and Russian interest appears high, with much political weight attached to these engagements. The Daily Maverick has reported that the Russian government has offered 300 million doses of the Sputnik vaccine, with financing, to the African Union and that the Chinese government has pledged almost 25% of all its vaccine donations to the continent. As already stated, NDoH officials have engaged in talks with Russian and Chinese COVID-19 vaccine producers. However, procurement of the Russian-made vaccines has seemingly not been prioritised because, according to the Deputy Director General in the NDoH, Dr Anban Pillay, the NDoH “was concerned about the adenovirus 5 vector used in the [Sputnik] shot, which has in previous studies appeared to make people more susceptible to HIV infection.”
In November 2020, the Chinese ambassador to South Africa, Chen Xiaodong, was quoted as promising that China “shall give full play to South Africa’s important role as a bridge for BRICS cooperation with Africa.” Furthermore, they stated that “Under the guidance of BRICS public health cooperation, we shall promote the development of the BRICS Vaccine R&D Centre, advance collective vaccine research and trials of BRICS countries, including China and South Africa, set up plants, authorise production and recognise each other’s standards. We shall support Chinese enterprises in African countries including South Africa in conducting the Phase 3 vaccine clinical trials, and exploring the use of traditional medicine in the prevention and control of Covid-19, so as to help African countries defeat the pandemic at an early date.”
Health Minister Mhkize was quoted, in February 2021, as saying that the NDoH had “an interest” in the Sinopharm vaccine because it “appear[ed] very promising on available data”, and would consider the Sinovac and Sputnik V vaccines. On 10 March, SAHPRA announced it had received a dossier from Sinovac seeking regulatory approval, and on 29 March 2021, Daily Maverick reported that Sinovac announced that it will commit 5 million doses of CoronaVac to South Africa. However, at the time of writing this vaccine had not yet been granted approval for use in South Africa by SAHPRA. In the same month Mr Xiadong was quoted in the press as saying that Beijing was “willing to take stronger actions to support South Africa in overcoming Covid-19 and other difficulties, so as to better deliver post-Covid economic recovery and sustainable development”, though it is hard to know what this means in concrete terms.
Expectations Towards Other International Actors
Views on COVAX
One view, mainly from civil society globally but not strongly articulated in South Africa, is that COVAX is actually a hinderance to equity. This is because it cements market mechanisms, is non-transparent and has given unelected stakeholders decision-making powers that have life and death consequences. Local actors such as the Peoples Vaccine Campaign (PVC) believe it is important that international actors recognise the limits of COVAX and stop using COVAX as a rationale for opposing the waiver. If they do so, they are effectively opposing vaccine equity by postponing the development of local manufacturing capacity. A second view is that COVAX is already here and is here to stay, so it should be made to operate in ways that do not perpetuate vaccine inequity – for example, by ensuring transparency and an end to non-disclosure agreements (NDAs), more active involvement from civil society in decision-making and so on; Peoples Health Movement South Africa (PHM-SA) and other SA CSOs more or less support that view.
Expectations of International Actors
Northern governments have put substantial public funds into vaccine R&D but appear happy to allow private corporations to exploit the IP. This is to the disadvantage of populations in the global north and low- and middle-income countries (LMICs). The expectation is that northern governments should insist on being able to open up patent protections so that all populations are protected, whilst corporation are able to make fair profits, but not profits at the expense of people’s human rights. One way to do that is through supporting the WTO waiver, particularly now that the US has indicated that it is willing to move to text-based negotiations. Additionally, they should be putting funding into technology transfer, particularly to the global south, or making any public funding of private corporations pursuing vaccine development contingent on clear deliverables for technology transfer. More broadly, financing institutions should recognise the need to invest in production capacity in LMICs, including the importance of securing markets for local production.
Recommendations
Key recommendations:
- We need to recognise that IP is not an end in itself but is only worth protecting if it creates social benefit. Where it leads to social harms, we need to suspend it.
- Support the waiver of all COVID-19 diagnostics, treatments and vaccines, or at least do not oppose it.
- The waiver alone will not be enough: political, technical and financial support for technology transfer is critical. We need diverse sources of production in all continents, and across LMICs and high-income countries (HICs).
- In keeping with the International Covenant on Economic Social and Cultural Rights (ICESCR), parties to the covenant should fulfil their legal obligation to ensure their engagements in international trade, finance and scientific research promoting the right to health. Recognising vaccine access as a human right (see the Committee on Economic Social and Cultural Rights’ position) and vaccines as a public good is one aspect of this.
- The WHO should be strengthened as the lead agency coordinating all policies and mechanisms for distributing access to essential diagnostics, devices, treatments and vaccines during international health emergencies. WHO member states should have a meaningful role in these processes, and should ensure through their untied contributions that the WHO is sufficiently resourced to serve this role effectively.
- The recommendations of the UN Secretary General’s High-Level Panel on access to medicines must be implemented urgently to create a more just and transparent R&D landscape, greater medicine manufacturing capacity in the global south, and more equitable access to essential medicines and medicines. It is disturbing that these recommendations have been systematically ignored by the international community since their publication in 2016. Notable are recommendations aimed at limiting the very actions that have necessitated the TRIPS waiver request, namely:
- The inclusion of TRIPS plus provisions in trade agreements.
- Governments and the private sector imposing “explicit or implicit threats, tactics or strategies that undermine the right of WTO members to use TRIPS flexibilities”.
- Institutions that receive public funding not “prioriti[sing] public health objectives over financial returns in their patenting and licensing practices”.
- Lack of transparency from private sector companies regarding R&D, marketing, manufacturing and distribution costs, clinical trial data, and licensing and purchase agreements for their products with governments.
- Northern civil society organisations should lobby their governments for the above in order to:
- Facilitate speedier and more equitable access to COVID-19 vaccines globally – something that will have public health benefits in both the global north and the global south as “no one is safe until everyone is safe”.
- Promote structural changes aimed at improving and democratising global research, disease surveillance and medicine manufacturing capabilities in order to ensure a more effective response to future international health emergencies.
- Mobilise to ensure governments face political sanctions from their own voters if they neglect their human rights obligations. The COVID-19 pandemic, and HIV/AIDS pandemic before it, has shown that domestic lobbying and advocacy by civil society in the global north, in conjunction with actions by states in the global south and civil society, is crucial in ensuring that the voices of people in the global south are not systematically ignored.
